
Most theories indicate that prostate cancer thrives off of testosterone. These theories are debatable yet I believe that in many cases they have merit. So, as a first line of defense against the cancer, testosterone is reduced to low levels (<20 ng/dl). Associated with testosterone reduction is loss of muscle mass and libido, fat gain, loss of bone mass, and other undesirable changes. But those changes are often temporary since testosterone reduction might be cycled (6 months on, 6 off, or other timing periods). The prostate cancer goes into remission for a few years for some men. For a lucky few it is apparently in remission or gone for decades.
For over 40 years the reduction in testosterone was achieved primarily by increasing estrogens. This caused a biological response and the body reduced its production of testosterone. However, a major side effect was cardiac issues. Heart attacks and strokes were apparent in about 30% of the men going through estrogen therapy. Obviously, this was a major negative. So work was done to develop new methods to reduce testosterone. One that was deemed successful was a drug call Lupron. Lupron reduces testosterone, frequently to 20ng/dl (nanogram/deciliter) levels or even lower. Sometimes 50ng/dl or 100ng/dl levels are achieved with Lupron. Levels above 20ng/dl are associated with poorer outlooks from the cancer, but it was deemed superior to the cardiac risks inherent with estrogen.
Two of the main side effects of Lupron are loss of bone (osteopenia leading to osteoporosis) and also depression. Depression occurs in about 30% of the case studies but loss of bone mass occurs in over 80% of the men who have been studied.
My doctors wanted me to start Lupron for ADT. I have slight bone loss already and this did not seem ideal to me. They assured me that there were other drugs that could help with the bone loss and other drugs that would help with the side effects of those drugs and I could take more drugs if I became depressed. All in all, it seemed like a very bleak outlook for me. Lots of drugs and side effects or prostate cancer that might spread.
Faced with two poor choices I began to research alternatives. I found out that the cardiac risk of estrogen primarily affects those who might be at higher risk to begin with. Individuals who are overweight or have had prior heart issues are the primary targets of increased risk. The increased risk for people outside of this population is still non-zero but not as high. NIH researchers also found that oral estrogen is primarily responsible for the increased cardiac risk; whether one is in the higher risk category or not. By bypassing the liver the increased risk is reduced from 30% to somewhere in the neighborhood of 5%. And after 1-2 years of estrogens the risk of cardio events decreases significantly compared to the overall population (estrogen therapy actually becomes cardio protective). Bone loss is reversed. Instead, estrogens reliably increase bone mass. There is also little additional risk of depression. NIH researchers then studied the big question. Does non-oral estrogen therapy reduce testosterone? Their answer is yes. However Lupron has been firmly established and it is hard to unseat it.
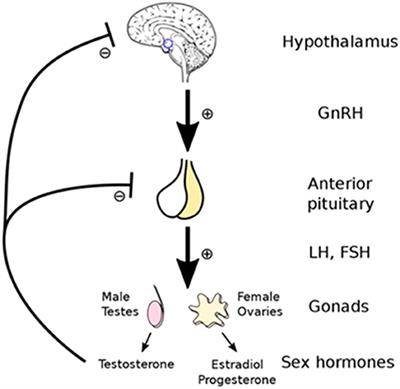
High estrogen works because it shuts off testosterone production. This is primarily due to a feedback loop. As E increases luteinizing hormone (LH) is reduced. LH stimulates T and E production. With no LH there goes T and endogenous E (E made inside the body). Unfortunately there too goes the stimulation for the leydig cells. So no sperm and no libido. We don’t seem to know how to get around this issue today.
E-ADT is more effective initially than standard ADT because most PCa has lots of ER-beta and little ER-alpha, and ER-beta helps to kill PCa. This treatment gives a selective growth advantage to those cells with lots of ER-alpha and little ER-beta which thrive in the presence of high estrogen, making this treatment counterproductive in time. I speculate that after 3-6 months of E-ADT it might be productive (if one desires to continue ADT) to switch to a lupron or relugolix ADT.
I decided to take a chance on estrogen therapy (I called it E-ADT). I chose the estrogen patch (other choices are creams and gels). I started with .5mg/day (milligram/day). After 2 weeks my testosterone had gone down but not sufficiently low (it was relatively high to begin, 1216 ng/dl, and had only dropped to 526ng/dl). I stuck with the estrogen but decided that if 250 ng/dl wasn’t achieved by week #6 and 50ng/dl wasn’t achieved by week #8 I wasn’t going to continue with it but would try Lupron instead.
I had my testosterone measured at week #6 and it was undetectable (threshold of the blood test I used is 3ng/dl). I reduced the patches to a dose of .3mg/day. As weeks passed it still was undetectable. So I reduced the dose to .1mg/day. My testosterone bounced back to 24 ng/dl. I increased the dose to .3mg/day and within a week it was undetectable again. Please note that right before I had my testosterone measured on week #6 I started Zytiga. Zytiga reduces testosterone. However I do not think that Zytiga would have acted within 24 hours.
As a side note I had no depression whatsoever. While I didn’t gain any fat I lost almost all nonessential muscle. My heart rate was around 45-50 bpm and my blood pressure hovered around 125/70.
I would love to see an ADT study showing prostate cancer survival vs. testosterone levels. The only studies that I have seen contrast 20ng/dl vs 50ng/dl and show superior survival in the 20ng/dl group. But that leaves me wondering what happens if you can decrease it even further.
This, as all medical decisions are, is a very weighty decision. Please fully research your options, get opinions, and then decide what you want to do. Monitor the results. Remember that I am only one individual and while it worked extremely well on me that does not mean that it will work for everyone. One of my naturopathic doctors would differ on that one – he is 100% convinced that it works on everyone and is far superior to Lupron. However, most doctors do not think that estrogen therapy will work to reduce testosterone.
Side effects:
- Muscle loss: this can be mitigated to some degree by weight-lifting.
- Libido: I don’t know how to change this one. I had 100% loss of libido when I was on E-ADT but after I stopped my libido came back.
- Hot flashes: a small dose of estrogen can help. Perhaps in patch form. I didn’t have a problem with hot flashes. But sometimes at night I felt flushed.
- Bone loss: again mitigated by weight-lifting.
- Gyno (breasts): my breasts grew. Went away completely when I stopped E-ADT.
- Fat gain: I didn’t have fat gain but rather fat loss. Going into the E-ADT I made the decision to try hard to keep from gaining fat. So I cut my calories by about a third and did lots of cardio and weight-lifting.
- Depression and fatigue: weight-lifting can reduce both of these. I didn’t have depression and not much fatigue.
Update 9/2019: I hated zero testosterone. I did not have depression, had some fat loss, and had no bone loss that I was aware of (too soon to test it but biology of estrogen indicates to me that, if anything, bone density should be increased over time). There was also no discernible change in my lipids or blood pressure. However I had no libido and my muscle was wasting away quickly. And it lowered my hemoglobin and white blood cells. So I looked for a way to block DHT (DHT is dihydrotestosterone and has an androgenic affect 3x-6x as powerful as testosterone and up to 10% of testosterone is converted to DHT). Originally I was thinking finesteride (proscar) to block the conversion from testosterone to DHT. But then I found dutasteride. Finesteride blocks about 70% of the conversion. Dutasteride blocks 90% at a dose of about 0.5mg/day.
Then I was trying to find the other piece of the puzzle: a way to block the androgen receptors in the prostate cells. Bicalutamide (Casodex) does this at a dose of about 150mg/day. As a bonus, after looking into the combination of bicalutamide and dutasteride I found that it is a recent addition to the conventional arsenal. It is particularly effective for locally advanced prostate cancer (my cancer type).
So I talked to my naturopath and my oncologist and explained what I wanted to do and why. They were both on board with it. So I switched. Because prostate AR is blocked and conversion to DHT is blocked each drug increases testosterone. The combination increases it approximately 2x. I monitored and indeed it was about 2250 ng/dl (about 2x my 56 year old baseline).
Note that bicalutamide increases testosterone but also increases estradiol. There is one estrogen receptor that helps kill prostate cancer cells but there are a couple others that help it grow. An AI such as anastrozole or letrozole can be used if gyno is an issue or if estrogen goes to high (estradiol > perhaps 30 pg/ml).
Update 5/2020: I discontinued the BD therapy and never went back to the estrogen therapy. My testosterone got up to 2250 mng/dl but because the androgen receptors were blocked there was no muscle gain. But there was also no PSA rise. After I stopped I went on high dose testosterone. My serum testosterone is around 2500 ng/dl, free is 45 ng/dl and bio-available is 1050 ng/dl. My PSA went up to 0.06 but back to zero a few months later. Libido and muscle came back. There are some theories that estradiol is primarily responsible for PrC growth. This makes some sense to me since when you have testosterone a portion of it is converted to estrogens via the aromatase enzyme. And by reducing testosterone to zero, you also reduce estrogen to a negligible amount and PrC cells die (for a while).
There are two main estrogen receptors. ERa and ERb. ERa is suspected to cause PrC proliferation. ERb is suspected to kill PrC (via apoptosis or programmed cell death). It is possible, although I have not been able to determine this, that application of exogenous (external) estrogen mainly activates the ERb receptors while endogenous (internal) estrogen mostly activates the ERa receptors. This would explain why estrogen therapy was used conventionally for decades. It was fairly successful in many cases yet carried cardiac risks (detailed above).
Also of note is that most large population studies that I have seen don’t show an increased risk with higher testosterone. Some show no change in risk, some show a slight positive change, some show a slight negative change. On balance I saw a very small negative correlation (therefore higher testosterone -> slightly less risk of PCa).
What confuses the issue is that the clinical trials and studies that I have seen that show that a normal testosterone level vs. a castrate level kills PrC do not adjust for estrogen. What I would love to see is a good trial or study of various Gleason ranges and PrC stages that compares testosterone injections (with an AI to block estrogen) to testosterone injections (without an AI) to a control to ADT to estrogen patches. I think that while this would be difficult to perform on humans, perhaps we could glean some information from animal experiments. If anyone knows about such data please let me know!
In the meantime I am going to continue with the testosterone injections. The evidence is shaky (update 12/2020 – considerably more evidence and I wouldn’t term it “shaky” now. My questions are should it be cycled? How often? Which men do well and who does poorly and can we tell?) but I would rather be wrong and live for 5 years as a man than 30 years as a woman (I mean no offense to women, I was born a man and am used to it and have no desire to be a woman).
In 2020 the government conducted a “PATCH” trial to show the efficacy of estrogen patches instead of Lupron. As of this writing the results are not in yet. I expect it will eventually show that exogenous estrogen works as well or better than Lupron.
Update: as of early 2021 some preliminary results from the PATCH trial show that estrogen patches are just as good or better than Lupron.

Leave a comment