
Prostate cancer feeds off of testosterone, glutamine, IGF-1, and also fat (however, advanced PCa switches it’s metabolism to more of a classic glucose driven one). Take away the fuel and it starves. But one of the issues in conventional medicine is that we tend to look at one thing at a time. Cancer is not quite that simplistic. Block one path and the cancer adapts and goes down another path.
Non-advanced prostate cancer is one of the only cancers that does not primarily use glucose for fuel. It is more fat driven. But blocking insulin (and therefore keeping blood glucose levels low) is still beneficial. There are substantial decreases in all cause mortality and, it is important to note, that many byproducts of glycolysis are used for the production of fatty acids (glycolysis is simply the production of pyruvate from glucose). The fatty acids fuel prostate cancer.
I doubt we know everything that prostate cancer can use for fuel. But we do know that if we reduce testosterone, fat, glutamine, IGF-1, and block certain estrogen metabolites (some are very protective and others introduce DNA mutations) we should be able to reduce mortality from prostate cancer.
An old diabetes drug that reduces the insulin spikes that lead to high blood sugar is metformin. This drug has been used by diabetics for years and is “relatively” safe.
Large studies show that mortality from aggressive prostate cancer is much reduced among diabetics who take metformin. 80% 10 year survival vs. 56%. The non-diabetic aggressive prostate cancer population has a 10 year survival of about 70%. Metformin performs this feat by attenuating insulin spikes. It is a blood glucose “normalizer”. This means that it rarely drops blood glucose to hypoglycemic levels. Yet it takes the spikes down.
There is a natural alternative to metformin that is supposedly just as effective (Berberine).
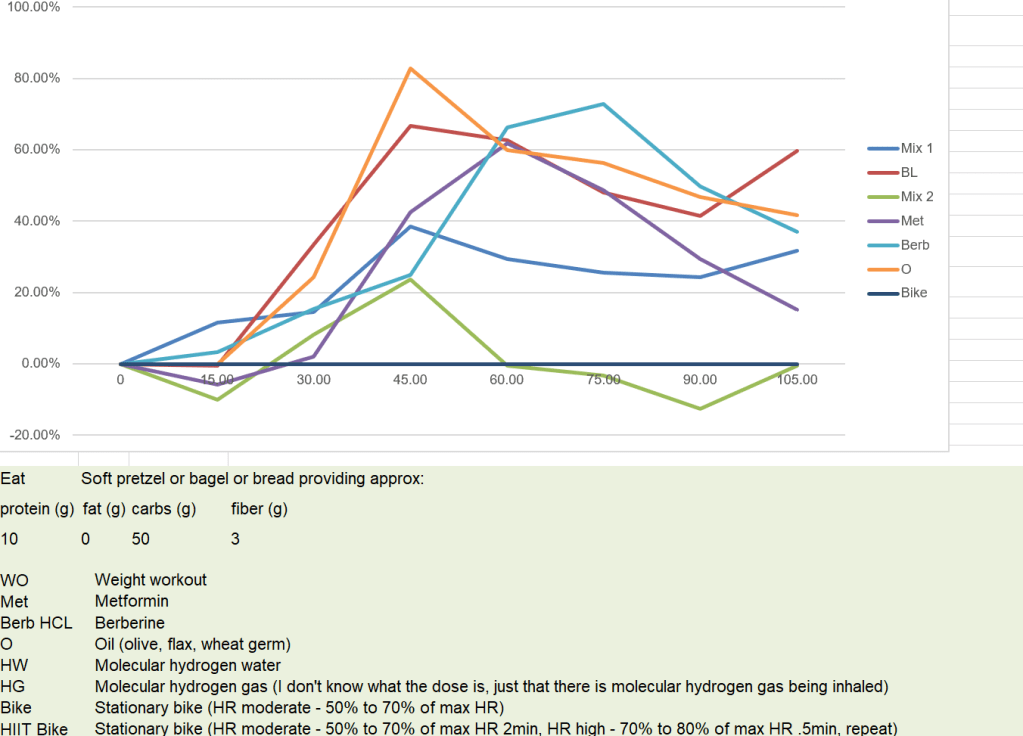
After collecting some data and deciding what the “glucose bullet” is, the bullet will be tested against a baseline with various meals. And then the baseline vs. bullet test will be repeated every month or so to make sure that habituation, coincidence, etc are not an issue. And there is always the distinct possibility that no meaningful data comes out of this study. If anyone has any comments or suggestions, I’d love to hear them! Also, if anyone wants to help me out and replicate the whole test on themselves or the “bullet” vs baseline, it would be great.




Just discovered that I have prostate cancer, literally yesterday. I go for a bone scan tomorrow, then meet with the Urologist to discuss treatment. Not ready for surgery just yet, just finished recovery from Aortic Valve replacement. Now this. Ultra Sound did not indicate caner on the surface, but the biopsy was positive. I’d be interested in learning all you know.
LikeLike
Do you know the gleason score yet? If the G score is 7 or less and it’s T2 or T1 it’s not a lot to worry about. If you have boys you’ll want to do some genetic testing on the tumor so that they know what their hereditary risk is and it likely guides lifestyle and treatment options for them.
In my case a biopsy showed that it was tiny, confined the prostate, and a G7, T2. I opted for surgery (RP) to remove it. Glad I did because something happened between the biopsy and surgery. It was a G9, T3, local lymph node positive. Even so I have about a 100% chance of living for 5+ years.
LikeLiked by 1 person
I don’t really know anything yet, just that it there. My ultrasound with the biopsy didn’t even give the Urologist any indication of cancer, until the biopsy came back. Hopefully that mean its contained within my prostate. Will know more after the bone scan. Don’t know the gleason score yet. Urologist didn’t say much over the phone. Just set up the bone scan. Thanks for your feedback and hope you are doing well!
LikeLike
I’m doing well. Thanks! Hope you’re doing well also.
This is just speculation but I think that when cancer is prodded (biopsy) it becomes aggressive. I’ve seen some speculation on the web (doctors). I know that when I was biopsied mine was very low grade, minimal cancer (it was only found in 1 out of 18 cores and the DRE and MRI showed nothing). But then I researched for 5 months before doing a surgery (some doctor’s told me to do nothing – just watchful waiting or active surveillance). But fortunately I decided to get the surgery (I figured I wasn’t getting any younger and if I had to do something someday it might as well be now). When they did surgery it was found to be very invasive and aggressive.
My point is that if you decide to do surgery or ultrasound or cryo or whatever, I’d do it sooner rather than later. At the very least you’ll know what you’re dealing with and won’t have nagging doubts like I do.
LikeLike
So, I think you should start figuring out your game plan now rather than waiting for the biopsy results.
Personally I’d steer clear of radiation. Seemed like bad news to me and almost everyone I know of who has had radiation regrets it. Side effects take a few years to start to show but they can be bad.
LikeLike